Medicaid Managed Care Rule: Three Things Plans Should Know
Summary
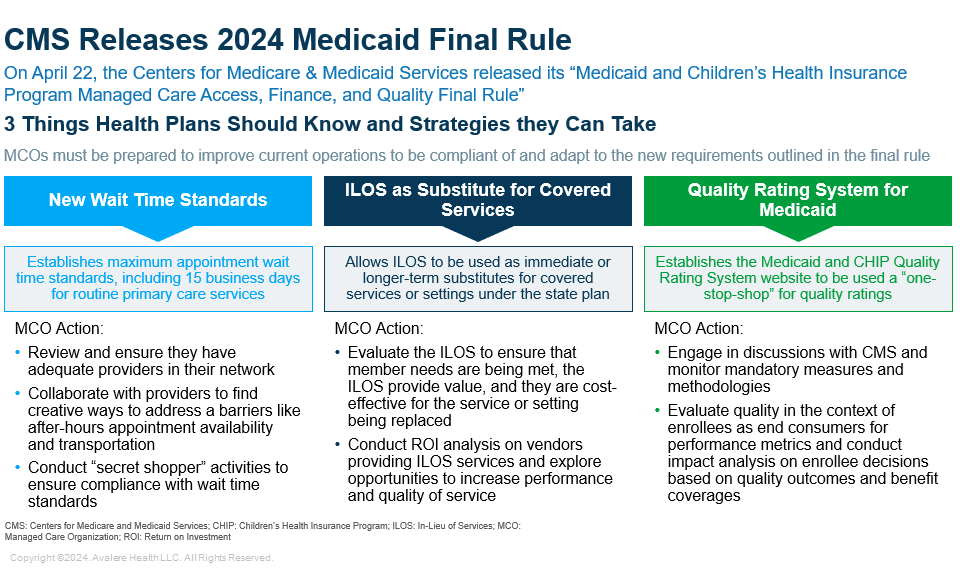
CMS’s new Medicaid and CHIP managed care rule will impact wait time standards, In Lieu of Service and Setting usage, and quality rating.On April 22, the Centers for Medicare & Medicaid Services (CMS) released its “Medicaid and Children’s Health Insurance Program (CHIP) Managed Care Access, Finance, and Quality Final Rule.” The rule demonstrates CMS’s continued efforts to expand access to Medicaid and CHIP managed care organizations (MCOs) while maintaining program quality. Below are three key operational areas the rule changes may impact:
1. Wait Time Standards
The rule establishes maximum appointment wait time standards, including 15 business days for routine primary care and obstetric/gynecological services, and 10 business days for outpatient mental health and substance use disorder services. This is the first time that CMS has required states to establish an appointment wait time for state-selected services, and states must use an independent entity to conduct annual secret shopper surveys to validate compliance, submit annual payment analysis comparing managed care plans’ payment rates and the state’s Medicaid payment rate, and conduct an annual enrollee experience survey for each managed care plan.
These changes mean that MCOs will no longer be able to consider their networks adequate based solely on the number of providers, but the ability to access the services of those providers as well. MCOs will need to ensure there are adequate providers with enough appointment slots in their networks to remain compliant with the new wait time standards. MCOs should collaborate with providers to identify barriers members might face when making appointments and find creative solutions to address those barriers.
For example, members might not have time for medical appointments during traditional business hours or they may not have adequate transportation to those appointments. MCOs can implement strategies such as working with providers to incorporate after-hours and/or weekend appointments into value-based contracts or expanding transportation benefits for enrollees. Finally, MCOs can establish a monitoring dashboard based upon independent evaluation findings for “secret shopper” activities to ensure that their network complies with the required standards.
2. In Lieu of Service and Setting as Substitutes for Covered Services
CMS specified that In Lieu of Service and Setting (ILOS) can be used as immediate or long-term substitutes for covered services or settings under the state plan. Since 2016, CMS has enabled MCOs to use ILOS to employ innovative options to reduce health disparities and address health-related social needs, such as housing instability and nutrition insecurity. In the new rule, the approval process can be done through the state Medicaid plan or a 1915 (c) waiver, but specific information must be documented in the managed care plan contract for each ILOS.
MCOs need to consistently monitor the ILOS they offer to ensure that member needs are being met, that the ILOS provides value, and that the ILOS used is cost-effective for the service(s) or setting(s) being replaced. For example, if a food delivery service is being used to replace a nutrition benefit, the MCO must review the program using implementation science and evaluation methods to ensure that the service is being delivered and used as intended and generating a return on investment (ROI) compared to a nutrition benefit. MCOs should also conduct ROI analysis on vendors providing ILOS and explore opportunities to increase performance and quality of services as needed.
3. Quality Rating System for Medicaid
CMS finalized its proposal to establish the Medicaid and CHIP Quality Rating System website to be used as a “one-stop-shop” for beneficiaries to compare the quality and key features of Medicaid plans, such as formulary and provider network. The agency will establish a framework with mandatory measures and methodologies for ratings calculations in future rulemaking.
MCOs should continue to monitor CMS for updates on mandatory measures and methodologies for rating calculations and actively engage with CMS in discussions. More importantly, MCOs should explore quality performance in the context of enrollees as the end consumer of that data. The publicly available quality performance will change the dynamics of how quality performance is displayed and interpreted and may impact how enrollees make decisions when selecting Medicaid plans. MCOs will become more impacted by their quality outcomes and should carefully evaluate specifications of measures to ensure that they adapt to this expanded audience for quality scores.
To learn more about how health plans can implement changes from the final rule and how Avalere can help, connect with us. Download a summary of this Insight here.
{kind=link}
January 23, 11 AM ET
Learn MoreServices
produces measurable results. Let's work together.


