Utilization and Spending by Medicare Beneficiaries in Employer Part D
Summary
An Avalere analysis finds that, on average, non-LIS Medicare beneficiaries in Employer Group Waiver Plans (EGWPs) have higher utilization but lower out-of-pocket (OOP) costs than non-EGWP enrollees.Background
Under the Part D program, Medicare beneficiaries can purchase prescription drug coverage offered by private health plans in their area. Employers and unions can also provide Medicare Advantage and Part D coverage to their Medicare-eligible retirees through specialized plan known as Employer Group Waiver Plans (EGWPs). In addition to allowing EGWPs to restrict enrollment to their retirees, the CMS provides EGWPs with other flexibilities that allow these plans to offer more customized benefits and to provide coverage similar to what is offered to current employees.
Since the Affordable Care Act (ACA), more employers have been offering drug benefits to retirees through EGWPs, largely due to the ACA’s elimination of the tax deduction for employers receiving the Retiree Drug Subsidy (RDS).1 As a result, the number of employers receiving RDS has declined considerably and enrollment in EGWPs has increased. In 2018, 7.0M non-LIS beneficiaries were enrolled in EGWPs offering prescription drug coverage (22% of all non-LIS Part D enrollment).2
Drug Utilization and Spending Patterns
Generally, EGWP enrollees’ experiences in Part D differ from beneficiaries in standard Part D plans. These differences may be due to several factors. While all EGWPs offering prescription drug coverage must meet the minimum standard of benefits established in law, many EGWPs offer more generous coverage with lower cost sharing compared to standard Part D plans. Additionally, separate CMS guidance for employers offering these types of plans (e.g., flexibilities for EGWPs to offer more customized benefits for certain groups of enrollees) and differences in the populations enrolled in EGWPs (e.g., demographics, health status, income) compared to standard Part D plans may lead to different utilization and spending patterns for EGWP beneficiaries compared to those not in an EGWP.
Avalere’s analysis finds that, on average, compared to non-EGWP enrollees, EGWP enrollees filled more prescriptions in 2018 (27 prescription fills vs. 25) and had higher annual drug costs ($3,882 vs. $2,257). However, despite having higher utilization and drug costs, EGWP enrollees had lower annual out-of-pocket (OOP) spending on average ($379 vs. $517).
| EGWPs | Non-EGWPs | |
|---|---|---|
| Share of Beneficiaries with Any Utilization | 95% | 93% |
| Average Number of Prescriptions | 27 | 25 |
| Average Annual Drug Costs | $3,882 | $2,257 |
| Average Drug Cost per Prescription | $145 | $90 |
| Average Annual OOP Costs | $379 | $517 |
| Average OOP Cost per Prescription | $14 | $21 |
| Average Share of Drug Costs Above the Catastrophic Threshold | 22% | 34% |
Note: Data reflect utilization and drug costs across all non-LIS enrollees, including those with no utilization.
These trends are consistent across most top therapeutic areas by total spending. For example, for beneficiaries taking antidiabetics—the top therapeutic area for both EGWP enrollees and non-EGWP enrollees by total spending—EGWP enrollees had an average of $3,087 in total drug costs compared to $1,761 for non-EGWP enrollees. However, EGWP beneficiaries paid $216 on average in OOP costs for antidiabetic medications while non-EGWP beneficiaries spent an average of $324 OOP.
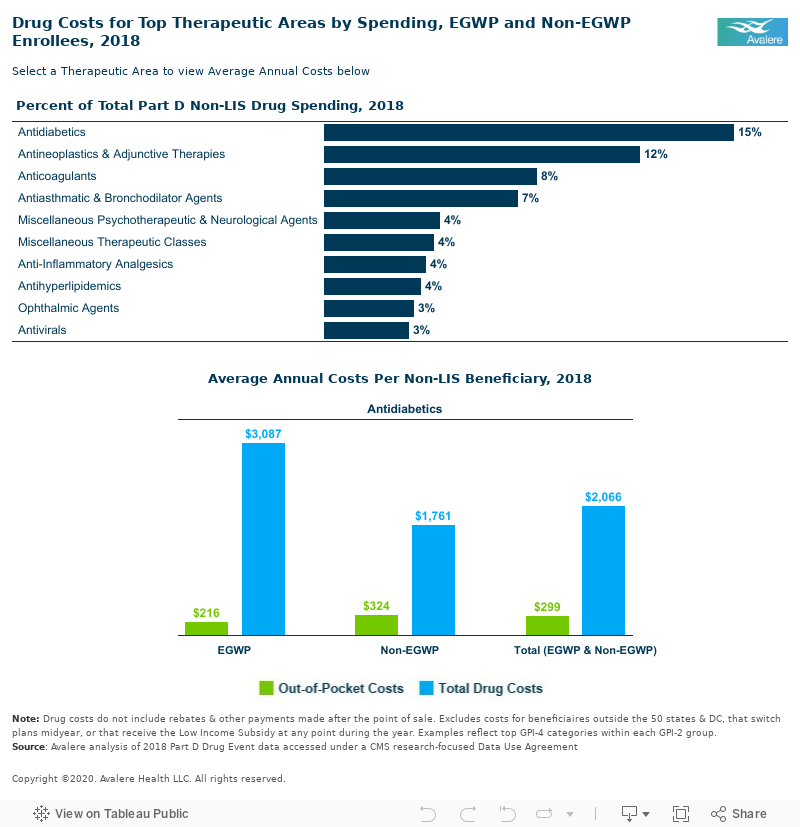
Drug costs do not include rebates and other payments made after the point of sale.
Methodology
Avalere analyzed 2018 100% Medicare Part D Drug Event data under a CMS research-focused data use agreement. Avalere used the Master Beneficiary Summary File to identify beneficiaries who were enrolled in Part D plans during the 2018 plan year. Beneficiaries with any month of LIS enrollment were excluded, as were beneficiaries who resided outside the 50 states and DC or changed plans mid-year. Avalere then identified EGWP and non-EGWP enrollees and took a random sample of each population such that the total sample drawn in each year was less than 20% of the Part D population. Avalere then summarized utilization and costs for each group, EGWP and non-EGWP, both overall and by therapeutic area (based on 2-digit Generic Product Identifiers from the Medi-Span database).
To receive Avalere updates, connect with us.
Notes
- Instead of offering coverage through EGWPs, employers can also receive the RDS from the CMS for offering creditable prescription drug coverage to retirees in group health plans. The ACA eliminated the tax deduction for employers receiving the RDS beginning in 2013.
- Estimates exclude beneficiaries with any month of LIS enrollment, beneficiaries who resided outside the 50 states and DC, and beneficiaries who changed plans mid-year.
Services
produces measurable results. Let's work together.


