Medicare Nebulizer Use for COPD Differs by Race/Ethnicity
Summary
Rates of filled prescriptions for nebulizers in Medicare FFS vary across factors such as age, disability, and race/ethnicity.Chronic obstructive pulmonary disease (COPD) is a common respiratory condition often requiring medication to ease difficulty in breathing. Inhalers and nebulizers are used to deliver medication. Because nebulizers do not require the same precise timing and dexterity as inhalers, they may be easier to use for patients with cognitive or neuromuscular impairments (often older patients and those with disabilities).
Avalere’s analysis of nebulizer prescription claims in 2021 Medicare fee-for-service (FFS) claims found an association between higher rates of nebulizer use and beneficiaries who are older or have a disability, compared to Medicare beneficiaries age 65-75 without a disability. Results also suggested differences in filled nebulizer prescriptions by race, regardless of disability and age. In 2021, there was greater nebulizer use among FFS Medicare beneficiaries with COPD who were White compared to those who were Black, Hispanic, Asian, or North American Native.
Background
COPD is a common chronic disease affecting roughly 11% of the Medicare population. The disease, which includes emphysema and chronic bronchitis, is characterized by restricted airflow and difficulty in breathing. To ease difficulty in breathing, individuals with COPD may require medication that is typically delivered through either an inhaler or a nebulizer. Both inhalers and nebulizers deliver medicine directly into the lungs but through different mechanisms. Inhalers use pressure to project aerosolized medicine into the lungs and the medicine is inhaled in through a mouthpiece. Nebulizers use a mask that fits over the nose and mouth to provide the medicine through a mist.
Both devices have benefits, and patients use them at different times. Inhalers provide immediate relief and are often used in the case of exacerbation. Exact dosing and correct use of an inhaler requires the user to fully inhale the medication, accurately time inhaler activation, and to hold the medication in the lungs before exhaling. Because of the coordination involved, patients with comorbidities affecting cognition or the neuromuscular system, or patients with a suboptimal peak inspiratory flow rate, may have difficulty properly using an inhaler. In contrast, nebulizers deliver long lasting inhalation therapy without requiring the same precision in delivery.
Avalere used 2021 Medicare FFS data to assess the use of nebulizers for the treatment of COPD. Compared to Medicare beneficiaries age 65-75 without a disability, older beneficiaries and those with disabilities may be more likely to have comorbidities affecting cognition or the neuromuscular system and therefore potentially higher rates of nebulizer use. This analysis also examined prescription claims for nebulizers by race/ethnicity and dual Medicare and Medicaid status to identify other potential disparities.
Analysis of Nebulizer Use in Medicare FFS Beneficiaries with COPD
Avalere identified over 1.9 million Medicare FFS beneficiaries with COPD in 2021 and found that 28% had a filled prescription for a nebulizer, including beneficiaries who had prescription claims for both nebulizers and inhalers (approximately 392,000 beneficiaries, or 20% of the COPD population).
Age and Disability
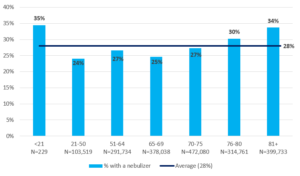
As hypothesized, the percentage of Medicare FFS beneficiaries with COPD and a filled nebulizer prescription was greater in older age groups, specifically beneficiaries over 76 years (Figure 1). Approximately 32% of beneficiaries with COPD over the age of 76 had a prescription claim for a nebulizer, compared to 28% in the overall COPD population.
Though Medicare beneficiaries with COPD under the age of 21 were a small percentage of the sample, they had a higher-than-average rate of nebulizer use (35%). The subgroup of beneficiaries under 21 was entirely comprised of beneficiaries enrolled in Medicare due to disability and the high rates of nebulizer use in this youngest population aligns with higher rates of nebulizer use in Medicare beneficiaries with disabilities (Figure 2).
Figure 1: Percentage of Medicare FFS Beneficiaries with COPD and a Nebulizer Prescription Claim in 2021, by Age Group
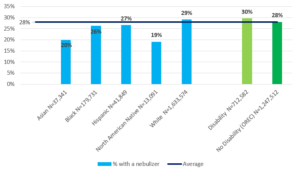
Beneficiaries with COPD who have a disability (as measured by the Original Reason for Entitlement Code [OREC]) had a higher rate of filled nebulizer prescriptions compared to those with no disability. Nearly one in four (36%) in the sample had an OREC code for disability, the proportion in this group with a filled nebulizer prescription was 29.5% compared to 27.5% in the group without disability (Figure 2).
Race / Ethnicity
This analysis also found differences in nebulizer use by race/ethnicity (Figure 2). The majority (84%) of the Medicare FFS population with COPD was White, 9% were Black, 2% Hispanic, 2% Asian, and 1% North American Native (remainder was missing or “Other”). Among White beneficiaries with COPD, 29% had a filled nebulizer prescription; use was lower for Hispanic (27%), Black (26%), Asian (20%), and North American Native (19%) beneficiaries with COPD.
Figure 2: Percentage of Medicare FFS Beneficiaries with COPD and a Nebulizer Prescription Claim in 2021, by Race/Ethnicity and by Disability Status
Predicting the Odds of Nebulizer Use: Multivariate Approach
In addition to the descriptive analyses reported above, Avalere conducted a multivariate analysis to examine the association between beneficiary-level characteristics and the odds of having a filled prescription for a nebulizer (logistic regression model developed using SAS statistical software). The results show a statistically significant association between disability (OREC) and nebulizer use. Patients with a disability had 51% higher odds in having a filled prescription for a nebulizer compared to those who did not have a disability, regardless of age and race/ethnicity. Each additional year of age was associated with a 2% increase in the odds of having a prescription claim for a nebulizer. Beneficiaries reporting race/ethnicity as Asian or North American Native were associated with lower odds of nebulizer use compared to beneficiaries who were White.
Table 1: Odds of Nebulizer Use with Confidence Intervals for Beneficiary Characteristics
| Effect | Odds Ratio | 95% Wald Confidence Limits |
|
|---|---|---|---|
| Dual Indicator | 0.986 | 0.979 | 0.994 |
| Age (years) | 1.022 | 1.022 | 1.023 |
| Disability (OREC) | 1.513 | 1.500 | 1.526 |
| Race/Ethnicity – Asian | 0.594 | 0.579 | 0.61 |
| Race/Ethnicity – Black | 0.881 | 0.871 | 0.892 |
| Race/Ethnicity – Hispanic | 0.906 | 0.886 | 0.927 |
| Race/Ethnicity – North American Native | 0.575 | 0.550 | 0.601 |
| Race/Ethnicity – White | Reference Group | ||
Conclusion
Older beneficiaries and those with disabilities had higher rates of nebulizer use compared to younger Medicare FFS beneficiaries. Regardless of age or disability status, the findings also indicate differences in nebulizer use by race/ethnicity where non-White beneficiaries had lower rates of nebulizer use compared to White beneficiaries. These findings support the hypothesis of greater nebulizer use among certain subgroups of beneficiaries and indicate potential disparities in access. Future analyses incorporating severity of illness or other factors could provide additional context for these findings. It will also be valuable to continue monitoring the use of the nebulizers as improvements in nebulizer technology and ease of use continue to evolve.
Methods
This analysis utilized the 100% Medicare FFS claims, accessed by Avalere via a research collaboration with Inovalon, Inc., and governed by a research-focused CMS Data Use Agreement (DUA). The sample included beneficiaries with COPD enrolled in Medicare Part A, B and D. Beneficiaries with COPD were identified through diagnosis or prescription claims. Identification by diagnosis required at least one inpatient visit or two outpatient visits with a COPD diagnosis (ICD-10 codes: J40-J44.9) in 2021. Identification by prescription claims required at least two claims for either inhalers or nebulizers in the year. National Drug Code and Healthcare Common Procedure Coding System were used to identify COPD enrollees by prescription claims. Race / ethnicity was defined using the Social Security Administration code for race on the Medicare claims.
Related Content

Services
From beginning to end, our team synergy
produces measurable results. Let's work together.
produces measurable results. Let's work together.


