More Low-Income Subsidy Enrollees Pay Part D Premiums in 2024
Summary
An Avalere analysis finds that from 2023 to 2024 the number of LIS enrollees paying a Part D premium increased by more than 1 million enrollees.Background
Medicare beneficiaries with low incomes (i.e., approximately $22,500 for an individual and $30,500 for a couple in 2024) and assets qualify for Part D premium and cost sharing assistance through the low-income subsidy (LIS) program. Beneficiaries who receive the LIS can enroll in certain standalone Prescription Drug Plans (PDPs) for a $0 premium. These plans are known as “LIS benchmark plans.” Every year, the Centers for Medicare & Medicaid Services (CMS) designates certain standalone PDPs as LIS benchmark plans in each Part D region based on the plan’s premium amount. A PDP can qualify as an LIS benchmark plan if it is a basic plan¹ and its premium is below or within a certain dollar threshold² of the weighted average of all Part D plan premiums in the region. By statute, Medicare Advantage Prescription Drug plans (MA-PDs) cannot be LIS benchmark plans, although their bids are included in the LIS benchmark calculation.
Those with LIS can choose to enroll in any Part D plan, including a LIS benchmark or non-LIS benchmark PDP or a MA-PD. However, beneficiaries with LIS who enroll in non-benchmark plans may have to pay a monthly premium. If a LIS enrollee does not actively select a plan on their own, CMS will automatically enroll them into a benchmark plan in their region.
Once an LIS enrollee joins a plan on their own, CMS will no longer automatically enroll or reassign them to a LIS benchmark PDP. LIS enrollees who are in a plan that no longer qualifies as a LIS benchmark plan for the following year will receive a letter from CMS. These letters state that they will have to pay a monthly premium if they remain in their current plan.³ However, these LIS enrollees must ultimately take action to switch to a different LIS benchmark plan in their region to avoid paying a premium.
Analysis Findings
A previous Avalere Insight detailed the decline in the availability of $0-premium LIS benchmark PDPs from 2023 to 2024. In this analysis, Avalere examined historic trends to assess whether the recent additional decrease in LIS benchmark plan options under the Inflation Reduction Act (IRA) correlates with more LIS enrollees paying premiums for their coverage.
Trends in LIS Benchmark Plan Offerings and Enrollment Patterns
Avalere found that the total number of $0-premium LIS benchmark PDPs across all states has declined steadily for the past five years, dropping by 15% on average from 2020 to 2024. However, the decrease in the number of LIS benchmark PDP options accelerated from 2023 to 2024, dropping by 34% (from 191 plans in 2023 to 126 plans in 2024).
Enrollment patterns have also shifted as the number of $0-premium LIS benchmark PDPs has decreased and as overall enrollment in Medicare Advantage has risen. In 2020, over half (54%) of LIS enrollees were in PDPs. Of these LIS enrollees in PDPs, 49% were in LIS benchmark plans. From 2020 to 2023, LIS enrollment in benchmark PDPs decreased by about 8% per year. The decline of LIS enrollment in benchmark PDPs further accelerated between 2023 and 2024. As of 2024, 34% of LIS enrollees are in PDPs, with 28% of these enrollees in LIS benchmark PDPs (Figure 1).
Figure 1. LIS Enrollment Across Plan Types and Average Premium Obligation, 2023 and 2024

Additionally, of the 4.6 million LIS enrollees in PDPs in 2024, CMS reassigned about 1.35 million (29%) enrollees to different $0-premium benchmark plans for the 2024 plan year. This reassignment occurred because the LIS enrollee did not join a plan on their own and their plan lost benchmark status in 2024, or their plan withdrew from the market. In previous years, CMS has reassigned about half a million or fewer enrollees annually.
LIS Enrollee Premium Obligations
As the number of benchmark PDPs has declined, the number of LIS enrollees in plans where they need to pay a premium has increased. In 2024, over half (56%) of LIS enrollees are in a plan where they are responsible for a monthly premium (Figure 1). Across all plan types (PDPs and MA-PDs), the total number of LIS enrollees who must pay a premium for their Part D coverage grew from approximately 6.4 million in 2023 to 7.5 million in 2024 (an increase of more than 1 million enrollees).
About 900,000 LIS enrollees are in non-benchmark PDPs and owe a premium in 2024. These enrollees owe an average premium of $34 a month, although some premiums are even higher. In 2024, over 120,000 LIS enrollees in non-benchmark PDPs have a monthly premium of $50 or more and about 25,000 have a monthly premium of $75 or more.
Meanwhile, more than 6.5 million LIS enrollees are in MA-PDs that have a non-$0 premium in 2024. LIS enrollees in these plans have lower premiums on average. However, more than 15,000 LIS enrollees in MA-PDs pay monthly premiums of $30 or more in 2024.
State Trends
Trends in enrollment and premium obligations for LIS enrollees in PDPs vary by state and by the availability of LIS benchmark plan options in each state. In 11 states, more than one-quarter of all LIS enrollees in PDPs are in non-benchmark PDPs (Figure 2). These states tend to have fewer LIS benchmark options, with 9 of the 11 states having three or fewer LIS benchmark PDPs in 2024. The maximum monthly premium obligation for an LIS enrollee in a PDP ranges from $61 in Oklahoma to almost $155 in Pennsylvania and West Virginia.
Figure 2. Percentage of LIS PDP Enrollees in Non-Benchmark PDPs, 2024
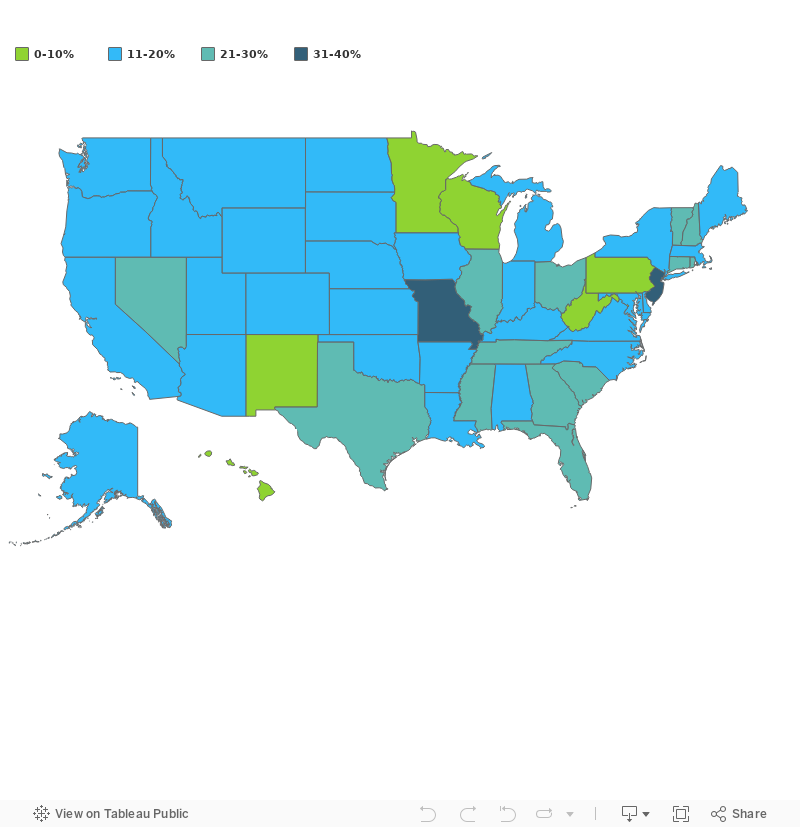
Note: FL, IL MO, NV, NJ, OH, and TX have 2 LIS benchmark options in 2024; however, 1 of these 2 plans is under sanction and cannot accept new enrollment, leaving enrollees in these states with effectively 1 LIS benchmark option.
Implications on LIS Access
The LIS program, as originally established by lawmakers, was intended to guarantee that beneficiaries with low income have access to $0-premium Part D drug coverage through LIS benchmark plans in addition to reduced or eliminated cost sharing. LIS enrollees, who represent some of the most vulnerable beneficiary groups, rely on these subsidies to ensure they have coverage for their prescription drugs. Compared to the overall Medicare population, those with LIS are more likely to have a disability, and/or multiple chronic conditions. Further enrollment in the LIS program is disproportionately comprised of those from racial and ethnic minority groups, including Black, Hispanic, and Asian beneficiaries.
In recent years, changes in the landscape and availability of plans, broader Medicare enrollment patterns, and other policy rules have shifted enrollment patterns of LIS enrollees. More recent policy and market changes have led to fewer LIS benchmark options in 2024 and more LIS enrollees paying premiums for their Part D coverage. As the most significant Inflation Reduction Act Part D benefit changes go into effect in 2025, the potential for even larger changes in plan offerings and enrollment are likely to have important access and affordability implications for LIS enrollees.
Methodology
Avalere’s analysis leveraged CMS’s enrollment and landscape files from March for calendar years 2020–2024. Avalere derived LIS enrollment using the Contract-Plan-State-County (“CPSC”) level Part D enrollment file released by CMS. Premium obligations for LIS enrollees in non-benchmark PDPs and non-$0 premium MA-PDs are reported for beneficiaries who received full premium assistance. PDPs meeting the de minimis were included in the analysis as LIS benchmark plans. Reported averages are not enrollment weighted. Results reported from the analysis exclude territories, and Employer, Cost, Medicare-Medicaid, and Program of All-Inclusive Care for the Elderly plans.
To learn more about the impacts of Part D market changes, connect with us.
Funding for this research was provided by the National Hispanic Council on Aging. Avalere retained full editorial control.
¹ Basic plans are actuarially equivalent (i.e., same generosity of benefits) as the defined standard Part D benefit set in law.
² This threshold is known as the “de minimis” amount and is set at $2 for 2024.
³ CMS sends notices to LIS enrollees who joined a plan on their own and will have a new or increased premium liability relative to the previous year.
Related Content


Services
From beginning to end, our team synergy
produces measurable results. Let's work together.
produces measurable results. Let's work together.


